Safety from the outside to the inside
Apr 2020
Written by Noel Macnamara
Being able to feel safe with other people is probably the single most important aspect of mental health; safe connections are fundamental to meaningful and satisfying lives
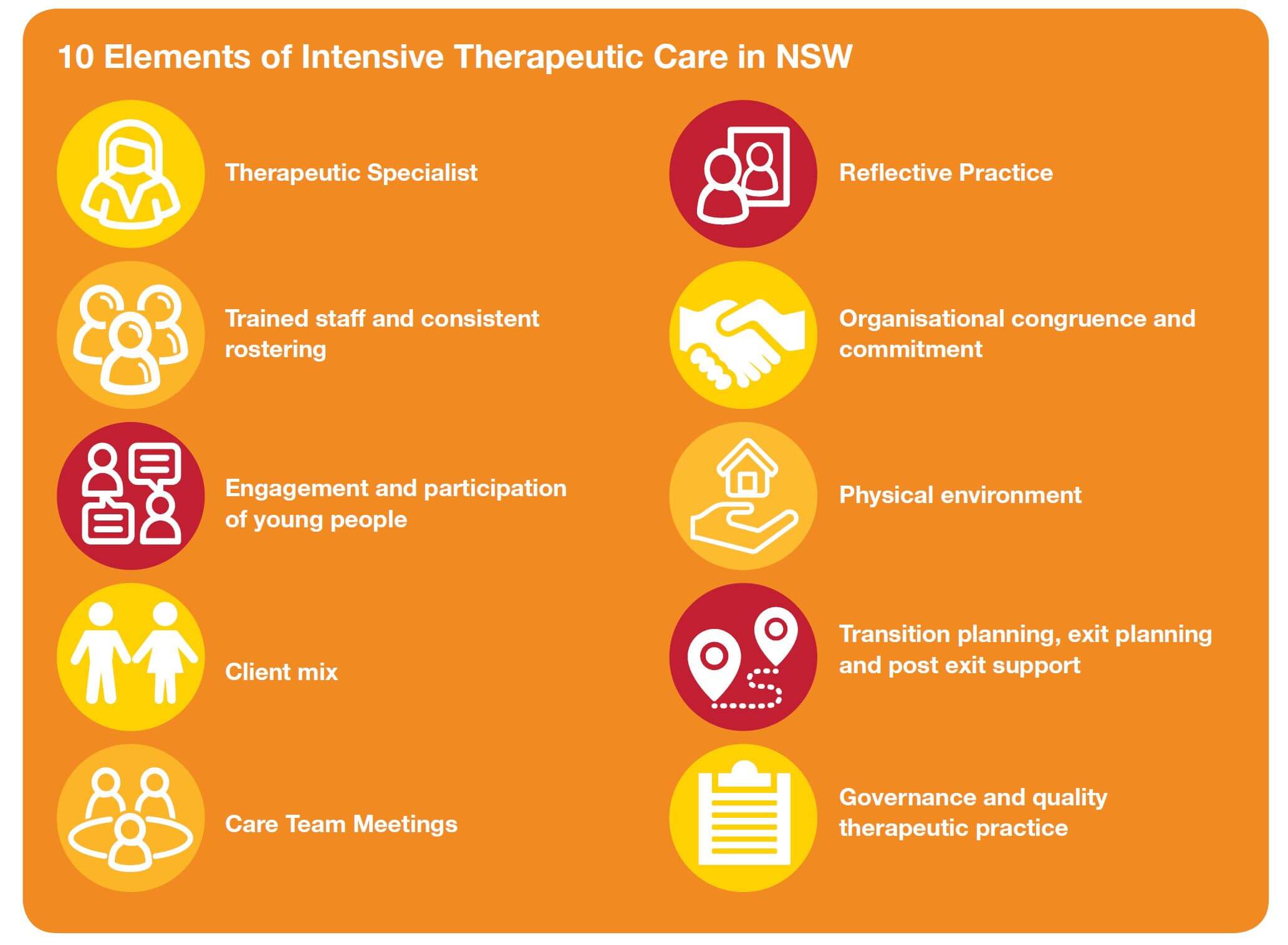
At the recent Therapeutic Specialist’s forum, there was lots of discussion about the concept of physical and relational safety in Intensive Therapeutic Care (ITC). We all agreed that it is a fundamental right of every child and young person in residential care to be and feel safe. Sadly, however, the reality is far from that, but it’s something we strive for nonetheless.
Safety is an important theme in healing, growth, and recovery from trauma. The very core of what the ITC system is attempting to achieve. Most of the children and young people in ITC have experienced trauma, abuse and neglect have lost their sense of safety. They need support to access appropriate tools and resources to return to a sense of safety.
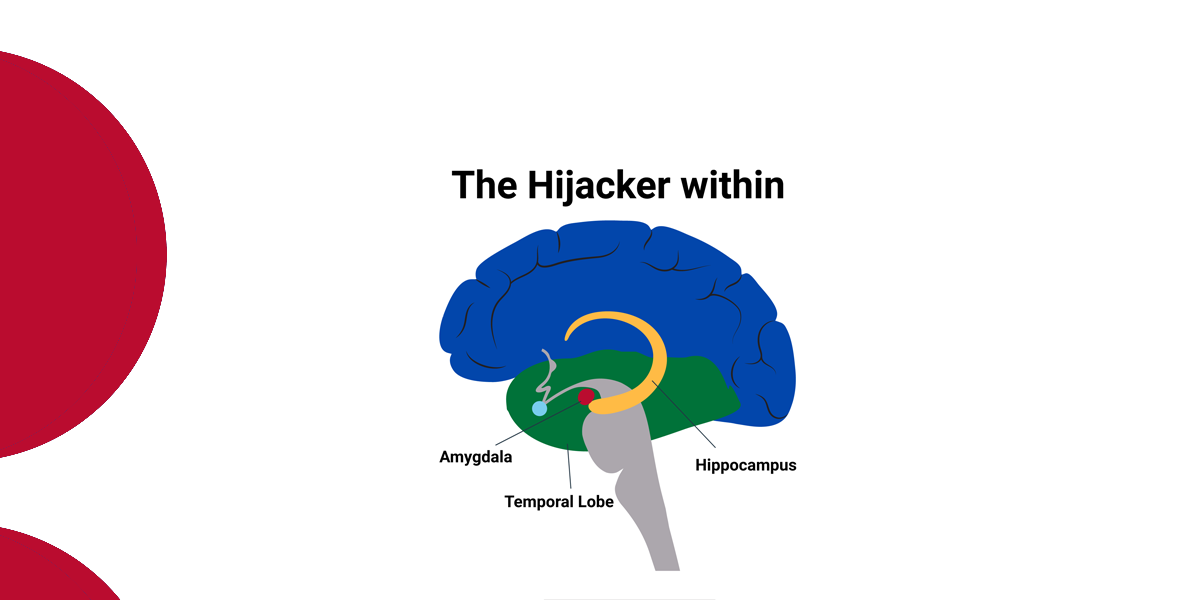
Feeling unsafe externally and/or emotionally limits the ability of children and young people to experience human connection, which is foundational to their wellbeing as social beings. When they don’t feel the benefits of meaningful relationships, their stress response system is continually activated. Over time repeated activation of the stress response takes a toll on the body.
Research suggests (Yaribeygi, Panahi, Sahraei, Johnston, & Sahebkar, 2017) that chronic stress contributes to high blood pressure, promotes the formation of artery-clogging deposits, and causes changes that may contribute to anxiety, depression, and addiction. Chronic stress keeps the system activated, much like a motor that is idling too high for too long. This is the essence of what the Adverse Childhood Experience research (Centres for Disease Control and Prevention, 2014) found. The impact of the stress associated with trauma abuse results in shortened life spans.
What does it mean to feel safe?
“Safe” is a hard-to-define experience, but something that we all know when we feel it.
Relational Safety
Relational safety is the knowledge and understanding residential staff have of a child or young person and of the environment, and the translation of that information into appropriate responses and therapeutic care.
Relational safety is not simply about having ‘a good relationship’ with a child or young person. Safe and effective relationships between residential staff and children and young people must be professional, therapeutic and purposeful, with understood limits. Limits enable residential staff to maintain their professional integrity and say ‘no’ when boundaries are being tested.
There are Two Main Facets of Relational Safety:
- The physical and emotional boundaries of the child or young person are respected. They can say “no”. A total contrast to their previous lived experience.
- They can have confidence that their physical and emotional boundaries will be respected and when there are reasons to not believe this is true, they can feel unsafe. Once again, a total contrast to the prior lived experience of the majority of the children and young people in ITC.
Here’s Another Way to Define Relational Safety:
- emotionally unsafe: receiving insults, shaming, bullying, threats, manipulation, dismissal of their thoughts or feelings, blame, receiving or seeing someone’s lack of emotion management but instead directing them towards others
- emotionally safe: a pattern of experiencing empathy, support, honesty, respect, and clarity
But feeling safe isn’t just about external, relational safety. It’s also an internal experience (given the right environment).
How can we help to build safety?
When someone has been in unsafe mode for a long time, like the children and young people we work with, returning to a sense of safety takes time and focused intention.
Ensure true safety
The most obvious first step is to ensure that the children and young people are, in fact, safe. Actions speak louder than words. Young people report that staff who are actively involved in their lives, particularly when they were able to engage with young people at their developmental levels made them feel safe. Having a strong presence and involvement in the day-to-day activities is important. Physical proximity and active involvement of residential care practitioners carry a more significant meaning for children and young people, one that is linked with their need for safety and connection.
Children and young people’s experiences in residential care settings are shaped not only by how residential staff act to protect them in times of need, but also how they bring control and structure to their day-to-day living environments. For young people who have experienced trauma, abuse and neglect in the past, a lack of control and structure in the residential care environment can be a significant trigger for retrieval of traumatic memories.
Establish and build relational safety
Secondly, children and young people living in prolonged fear states are often opposed to adult intervention, because they feel anxious about putting their faith in others; specifically, to trust the notion that there are safe adults.
When you haven’t felt safe for a long time, you might struggle with it even with a truly safe person. There can be so many factors that impede this process, so sometimes the structure, containment, and expertise of a therapeutic relationship is the needed first step for establishing feeling safe.
Key relational safety (Gunderson, 1978) features include:
Containment occurs when one person receives and understands the emotional communication of another without being overwhelmed by it, processes it and then communicates understanding and recognition back to the other person. This process can restore the capacity to think in the other person (Douglas, 2007, p.33).
This concept can also be applied to the more complex network of relationships amongst and between staff, children and young people in ITC. Containment involves directly addressing via verbal interpretation – Also involves the use of daily activities, transitions, leisure time, and even the physical environment towards the development of a containing atmosphere in which children and young people feel (over time) accepted, respected and understood.
Structure
Most children, especially adolescents, thrive in structured and predictable situations. Rules offer explanations about which behaviours are appropriate and what is expected of us. They also define boundaries, without which the world would feel chaotic and unsafe. In addition, rules take the emotion out of the equation and tell us what is expected.
According to Severe, 2004 there are three factors to consider when developing expectations or rules. Expectations must:
- Specific
- Reasonable
- Enforceable
Structure helps create a sense of relational and physical security. In the same way, the residential space needs structure – not just the building features, although they definitely help – but reliable routines and realistic rules and boundaries, in order for it to be a holding and healing place.
Support
Support functions to make a child or young person feel better and to enhance their self-esteem. Support can be given by accommodating to the child or young person’s limitations (e.g., acknowledging their developmental age rather than their chronological age). Support starts with a recognition of the child or young person’s pain-based behaviours. Support is most obvious when it consists of praise or reassurance.
Involvement
Involvement evolves from the structured interpersonal interactions with residential staff and other young people in the ITC house. Involvement strengthens tolerance for interpersonal relationships and helps to identify and modify individual relational challenges that the child or young person exhibits. Examples include: development of shared goals and collaboration case and therapeutic planning processes. All group activities make involvement a central process, especially during which a discussion of the group member’s way of relating to one another.
Validation
Many skills go into building safe relationships. One of those skills is the ability to validate others—to respond to the emotional experience of the child or young person with acceptance and understanding even if you don’t share their views. Validation is the ability to emotional track the child or young person which allows them to feel supported, accepted, and recognised, this process of validation in no way requires the staff member to agree what is being said by the child or young person. The process of validation creates a sense of safety.
Establish and build internal safety
Finally, having not learned in their earliest relationships how to self-soothe or manage their internal world; the children and young people in the ITC system need to develop the skills necessary to reassure themselves that the storm is not so frightening, that the worst-case scenario is not so terrible and that they have done the best regardless of the outcome.
To do this we must help them to develop emotional regulation, relaxation, communication and relationship skills (including facing conflict), practicing healthy boundaries, increasing physiological awareness, self-compassion and practicing self-care.
Conclusion
As we know feeling unsafe is deeply troubling, yet so many of the children and young people in the OOHC system live with being in that state most of the time, so much so that it feels normal to them.
The first and most fundamental goal of the ITC system is to create an environment (both a physical and relational space) that reduces anxiety and enables children and young people to feel emotionally and physically safe, especially when in crisis. So, they are able to face and work through their difficulties and engage in their healing journey.
All this means growing our staff, knowledge, skills, and tools for helping children and young people achieve an internal and external feeling of safety.
Noel MacNamara
Senior Advisor, Centre for Excellence in Therapeutic Care
References
Centres for Disease Control and Prevention (2014). The Adverse Childhood Experience (ACE) Study.
John G. Gunderson (1978) Defining the Therapeutic Processes in Psychiatric Milieus, Psychiatry, 41:4, 327-335.
Yaribeygi, H., Panahi, Y., Sahraei, H., Johnston, T. P., & Sahebkar, A. (2017). The impact of stress on body function: A review. EXCLI journal, 16, 1057–1072. https://doi.org/10.17179/excli2017-480.