The role fear plays in the lives of children and young people in out-of-home care
Aug 2023
Written by Noel Macnamara
Fear is a fundamental human emotion triggered by a perceived threat. It serves as a basic survival mechanism that signals our bodies to respond to danger with a fight, flight, or freeze response. As such, fear is an essential part of keeping us safe.
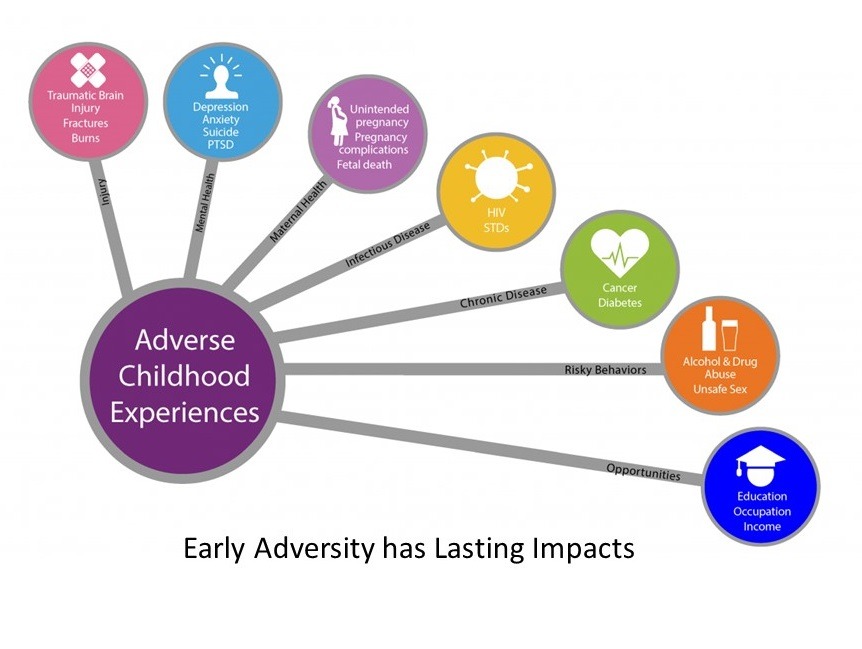
Typical childhood fears tend to disappear as children grow older. However, traumatic events that induce fear, such as physical and sexual abuse or exposure to family violence, contribute to lifelong impacts on well-being. Trauma affects the coordination of nerve networks. Adaptation to trauma, especially early in life, becomes a “state of mind, brain, and body” around which subsequent experiences organise (Cozolino, 2002). Abuse causes chronic stress on the brain. When threatening events that trigger fear are frequent and repetitive, the physiological responses to fear affect learning, behaviour, and relationships, as well as physical and mental health (Bromfield & Higgins, 2005, p. 39).
The National Scientific Council on the Developing Child at Harvard University (2010) puts it this way:
Science shows that exposure to circumstances that produce persistent fear and chronic anxiety can have lifelong consequences by disrupting the developing architecture of the brain.
In other words, our threat detection systems and subsequent feelings extend beyond assessing “is this dangerous?”, into numerous “what if” scenarios that include potential sources of harm.
The experience of fear as an emotion occurs because of the complex interaction between the activation of basic threat detection systems, memory storage and retrieval, and our own conscious awareness.
Removing a child from a dangerous environment alone cannot undo the serious consequences or reverse the negative impacts of early fear learning. There is no doubt that children should be removed from dangerous situations. However, simply moving a child out of immediate danger does not in itself reverse or eliminate the way that he or she has learned to be fearful.

How Fear Works
Fear prepares us to react to danger. Once we sense a potential danger, our body releases hormones that:
.
- Slow or shut down functions not needed for survival (such as our digestive system)
- Sharpen functions that might help us survive (such as eyesight). Our heart rate increases, and blood flows to muscles so we can run faster.
Our body also increases the flow of hormones to an area of the brain known as the amygdala, to help us focus on the presenting danger and store it in our memory.
Effect on the Key “Fear Centre” in the Brain
Two important structures in the brain, the amygdala and the hippocampus, have important roles to play on how the body responds to threat. The amygdala handles the brain’s response to stress, while the hippocampus helps process emotions and memories. Alterations in the amygdala can become the cause of future anxiety disorders.
Toxic stress hormones affect the growth of both the amygdala and the hippocampus. The stress hormone cortisol rises in relation to the level of trauma the child or young person undergoes and can become a cause of depression and aggression later in life.
Nervous Arousal
It is the amygdala that identifies potential threats, sending an alarm signal that is communicated to the rest of the body to prepare it for fight, flight, or freeze responses. This alarm signal is also sent to the brain structure responsible for judgement and reasoning, but this part of the brain is far slower to react – and for children who have experienced persistent fear of danger, it is often underdeveloped. Repeated traumatic experiences program the brain to quickly respond to danger, rather than developing the ability to thoughtfully use reason and logic to differentiate between threatening and non-threatening situations. Over time, living in persistent fear of danger develops an overactive stress response, and children become hypersensitive to normal stimuli – a touch on the arm, a smile, a tone of voice, a particular facial expression, or a smell could trigger this overactive stress response, to produce highly exaggerated fear reactions.
Effect on Brain Structure and Activity
Stress can reduce the volume of vital brain structures such as the hippocampus, corpus callosum, cerebellum, prefrontal cortex.
.
- The hippocampus is central to learning
- The corpus callosum is involved in higher cognitive abilities and emotions
- The cerebellum helps coordinate motor behaviour and executive functioning
- The prefrontal cortex is critical to behaviour, cognition, emotion, and social regulation, responsible for the majority of our rational decision-making, planning, and analytical abilities.
All these structures work together to help children and young people learn new things. However, chronic activation of the body’s stress response system damages their ability to learn and adversely affects brain architecture in these critical areas.
The Impact of Chronic Fear
Physical Health
Fear weakens our immune systems and can cause cardiovascular damage, gastrointestinal problems such as ulcers and irritable bowel syndrome, and decreased fertility. It can lead to accelerated aging and even premature death.
Memory
Fear can impair the formation of long-term memories and cause damage to certain parts of the brain, such as the hippocampus. Extreme stress increases the cortisol in our system (Murray-Close et al., 2008), which can interfere with hippocampus function and reduce its volume, leading to poorer declarative memory. This can make it even more difficult to regulate fear and leave a young person anxious most of the time. To a young person in chronic fear, the world looks scary, and their memories confirm that.
Brain Processing and Reactivity
Fear can interrupt processes in a young person’s brain that allow them to regulate emotions, read non-verbal cues and other information presented to them, and reflect before acting. This negatively impacts their ability to think and make decisions, leaving them susceptible to intense emotions and impulsive reactions. All these effects can leave them unable to act in socially appropriate ways.
In young people who have experienced trauma, fear signals are firing all the time. This does not require conscious influence – they often just feel constantly “on edge” for no apparent reason. They may have a sense of something being wrong, or of impending doom. These powerful feelings are generated deep inside the brain and cannot be eliminated by reason or understanding.
Mental Health Issues
Up to 90% of those who present to (public) mental health services have experienced physical, emotional, or sexual trauma (Cusack et al., 2006). Adolescents suffering fear associated with childhood abuse commonly experience mental health issues such as post-traumatic stress disorder (PTSD), conduct disorders, anxiety, mood disorders (including depression), eating disorders (including anorexia nervosa, bulimia nervosa, and binge eating), and personality disorders. Research also shows a strong link between childhood abuse and depression later in life (Christ et al., 2019).
Complicated Social Interactions and Learning Disabilities
Children and young people who have experienced the fear of trauma have difficulty interacting and relating to others, impacting their social interactions. When the primary relationship is one of betrayal, the child develops a negative set of beliefs, often struggling with other attachments throughout life. Many children and young people experience conflicted relationships and chaotic lifestyles. They often have trouble forming and maintaining relationships, as their reactions can disrupt close relationships (Henderson, 1977).
These children and young people are often mislabelled as having learning disabilities (Gilbert et al., 2009). The damage to structural and neurochemical development can affect executive functioning, resulting in lower academic achievement, intellectual impairment, decreased IQ, and weakened ability to maintain attention.

Helping Children and Young People who Display Fear-Based Responses
Responsive adults and caregivers can make all the difference for children and young people if they:
.
- Offer nurture
- Seek to understand before acting
- Interact with the child or young person at their emotional age
- Be consistent, predictable, and repetitive
- Model and teach appropriate pro-social behaviours
- Be available to listen and talk
- Have realistic expectations
- Be patient with the child or young person’s progress and with themself
- Take care of themself
What the children and young people in the out-of-home care system need most is to be surrounded by a healthy community that can buffer the fear, pain, distress, and loss caused by their earlier-life trauma. What works to heal them is anything that increases the number and quality of a child or young person’s relationships.
Recovery from the fear caused by trauma, abuse, and violence is also all about relationships — rebuilding trust, regaining confidence, returning to a sense of security, and reconnecting with others. Healing and recovery are impossible, even with the best medications and therapy in the world, without lasting connections to others.
References
Bromfield, L., & Higgins, D. (2005). National comparison of child protection systems (Child Abuse Prevention Issues No. 22). Melbourne: Australian Institute of Family Studies. Retrieved from www.aifs.gov.au/nch/pubs/issues/issues22/issues22.html
Christ, C., de Waal, M., Dekker, J., van Kuijk, I., van Schaik, D., Kikkert, M., Goudriaan, A., Beekman, A., & Messman-Moore, T. (2019). Linking childhood emotional abuse and depressive symptoms: The role of emotion dysregulation and interpersonal problems. PLoS ONE 14(2): e0211882.
Colozino, L. (2002). The Neuroscience of Psychotherapy: Building and Re-building the Human Brain. W.W Norton & Co.
Cusack, K. J., Grubaugh, A. L., & Knapp, R. G. (2006). Unrecognized Trauma and PTSD among Public Mental Health Consumers with Chronic and Severe Mental Illness. Community Mental Health Journal, 42, 487–500. https://doi.org/10.1007/s10597-006-9049-4
Gilbert, R., Spatz Widom, C., Browne, K., Fergusson, D., Webb, E., & Janson, J. (2009). Burden and consequences of child maltreatment in high-income countries. The Lancet, 373, 68-81.
Henderson, S. (1977). The social network, support, and neurosis: the function of attachment in adult life. British Journal of Psychiatry. 131(2), 185-191. doi:10.1192/bjp.131.2.185.
Murray-Close, D., Han, G., Cicchetti, D., Crick, N. R., & Rogosch, F. A. (2008). Neuroendocrine regulation and physical and relational aggression: The moderating roles of child maltreatment and gender. Developmental Psychology, 44(4), 1160–1176.
National Scientific Council on the Developing Child. (2010). Persistent Fear and Anxiety Can Affect Young Children’s Learning and Development: Working Paper No. 9. Retrieved from www.developingchild.harvard.edu