Untangling the challenges of FASD and trauma
Sep 2023
Written by Billy Black
In honour of FASD Awareness Month this September, the CETC brought together esteemed thought leaders Dr Julia Shekleton, Prue Walker, and Noel Macnamara to delve into the complex intersection between Fetal Alcohol Spectrum Disorder (FASD) and trauma. This panel discussion explored the ways we can integrate our understanding of FASD and trauma to better support and care for children within the out-of-home care system.

What is FASD?
From the NOFASD website:
Fetal Alcohol Spectrum Disorder (FASD) is the term used to describe the lifelong physical and/or neurodevelopmental impairments that can result from fetal alcohol exposure.
In simpler terms, children with FASD are born with brain damage and impaired brain growth due to their mother’s alcohol consumption during pregnancy.
One crucial point highlighted by the panel is the challenge of obtaining accurate data and information about the prevalence of FASD and the level of alcohol exposure in affected children. This difficulty is exacerbated by the stigma surrounding alcohol addiction and consumption during pregnancy and the fact that many mothers consume alcohol while unaware they are pregnant during the critical period of exposure.
What the data does show, however, is that FASD is a persistent risk marker for experiencing other ongoing childhood traumas, including neglect, physical and sexual abuse, family violence, and living in out-of-home care. When FASD and trauma are combined, they significantly amplify the risk of challenges with IQ, communication, memory, and emotional regulation.
Distinguishing between trauma-based and FASD-based behaviours
The panel also explored the challenges of attributing issues related to self-regulation to either trauma or FASD, and the subsequent difficulty of designing support strategies tailored to each child’s unique needs.
One significant hurdle is the frequent underdiagnosis or misdiagnosis of FASD, even when maternal alcohol use during pregnancy is known. Unfortunately, FASD is often considered an “invisible” disability. While some children with FASD may exhibit characteristic facial features, this visual evidence is only present in about 13% of diagnosed cases.
Dr. Julia Shekleton, a Clinical Neuropsychologist on the panel, noted that both FASD and trauma result in structural brain changes leading to difficulties in emotional and behavioural regulation. However, while children with a history of trauma may benefit from therapeutic interventions and show observable improvements in self-regulation, children with FASD face additional neurodevelopmental impairments that may significantly limit their progress. To effectively apply what they learn in therapy, children need skills in expressive and receptive language, reasoning, and the ability to apply new therapy skills to real-world situations — areas in which many children with FASD are often permanently impaired.
Children who seem to “refuse” to use their new behavioural strategies may receive other diagnoses such as Attention Deficit/Hyperactivity Disorder (ADHD) and Oppositional Defiant Disorder (ODD) for a long time before being accurately diagnosed with FASD. Due to associated issues with executive functioning, including attention and social skills, ADHD is one of the most common comorbidities seen with FASD.
Despite low recorded numbers of FASD diagnosed children, alcohol misuse plays a significant role in child protection assessments, and children in out-of-home care represent a high-risk population for FASD.
Understanding children’s capacities
A recurring theme throughout the panel discussion was the lack of awareness and understanding of FASD, which leads to unrealistic and unfair expectations of children’s support needs.
Most children with FASD encounter difficulties related to behaviour, attention, and social skills due to structural brain impairments. However, adults do not see this invisible impairment and often wrongly assume the child is “choosing” not to change their behaviour, failing to recognise that their brains may not have the capacity to progress in the same way expected of children without FASD.
FASD Specialist Prue Walker pointed out that children with FASD who have physical disabilities and impaired motor skills may receive more empathetic understanding from adults, despite sharing the same cognitive impairments associated with FASD. Due to the visibility of their symptoms, these children are rarely expected to “catch up” to their peers.
Children with FASD can often make some developmental and self-regulation gains when appropriate interventions are adjusted to their abilities and account for their unique brain structure. While we may not expect them to “catch up” to their peers, we can implement strategies that encourage incremental progress or finding workarounds for common issues, making developmental disadvantages less noticeable in daily life.
Matching support to children’s needs
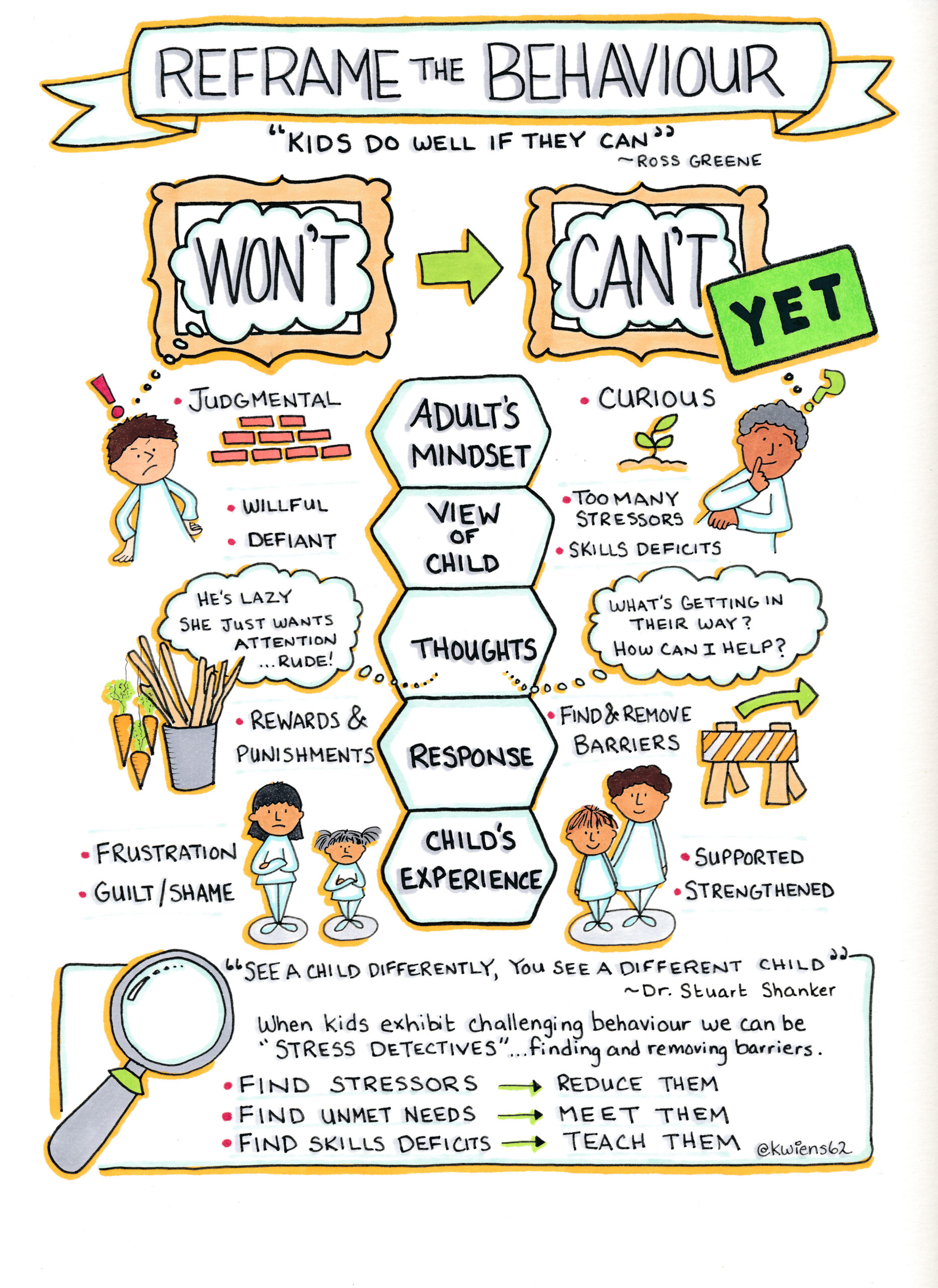
So, how can we approach children who struggle with emotional and behavioural dysregulation? The panel emphasised the importance of reframing our understanding of what children “won’t” do versus what they can’t yet do, given the right support to overcome their barriers.
When working with children diagnosed with FASD, there are ways to align our approach with the needs of brains with unique brain structure characteristics of FASD. Using consistent routines and repeating specific concrete instructions multiple times can help children retain what they’ve learnt in their long-term memory.
The “Eight Magic Keys” developed by Deb Evenson and Jan Lutke show that our approach to supporting children with FASD is not wholly dissimilar to how we approach supporting children who have experienced trauma – the key difference lies in narrowing our focus on simpler strategies and shorter-term goals.
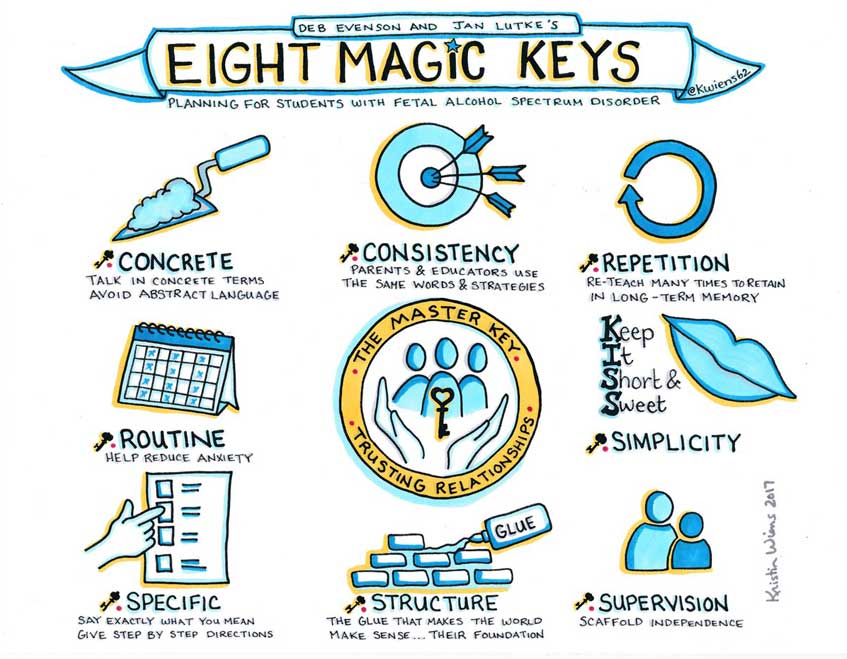
Above all, a safe trusting relationship with the child is key, as feeling safe is the most important first step towards developmental and emotional growth.
Resources
- If you are in Australia and suspect that a child that you work with or care for may have experienced prenatal alcohol exposure and has challenges consistent with FASD symptoms, you can start by consulting the child’s GP, requesting a referral to a FASD specialist through the FASD Hub’s service directory, or contacting the NOFASD Helpline on 1800 860 613.
- For those interested in watching the recording of CETC’s webinar Untangling FASD, Trauma, and Emotional/Behavioural Dysregulation, you can find it here.
- For more webinars and training workshops, please take a look through our CETC training website. You can also subscribe to the CETC newsletter to stay updated on our latest resources and training opportunities.