Interoception: the hidden sense that can help children understand their feelings before they react
Sep 2024
Written by Jessica Wright
You’re probably familiar with the five basic senses: taste, touch, smell, sight, and hearing. But did you know there are three additional ‘hidden’ senses that we use constantly to guide our bodies? These senses – proprioception, vestibular, and interoception – work together to organise how our body moves in space and interacts with our surroundings.
Proprioception is our sense of body position and movement through space. Using proprioception, we can feel our muscles contract and stretch, enabling us to consciously and unconsciously control our bodies without having to look. Proprioceptive input is highly calming and organising for our brain and body. If you’ve ever heard an Occupational Therapist refer to “heavy work” or “deep pressure” activities, these are proprioceptive-based activities.
Vestibular is our sense of head position, helping us control our balance, posture, and body during movement. Primarily located in our inner ear and brainstem, vestibular senses can be disrupted by stress and anxiety.
Interoception, the sense we will dive into today, is the sense that allows us to perceive internal bodily sensations, such as hunger, thirst, whether you need the toilet – and whether it’s urgent!
Interoception is highly subjective, and any person’s interoceptive accuracy can fluctuate throughout the day. There are known interoceptive profiles for those with neurodevelopmental differences such ADHD and autism (Garfinkel et al., 2016).
Interoception differences can be categorised into lower or higher interoceptive awareness, either of which can be problematic in different ways. Higher awareness may make children hypervigilant to body cues, which can make them prone to anxiety and overwhelm. Lower interoceptive awareness may result in missing body cues, resulting in overwhelm when those sensations become too strong to ignore.
Interoception and emotional self-regulation
The ability to recognise and respond to your internal sensations is the foundation for self-regulation skills.
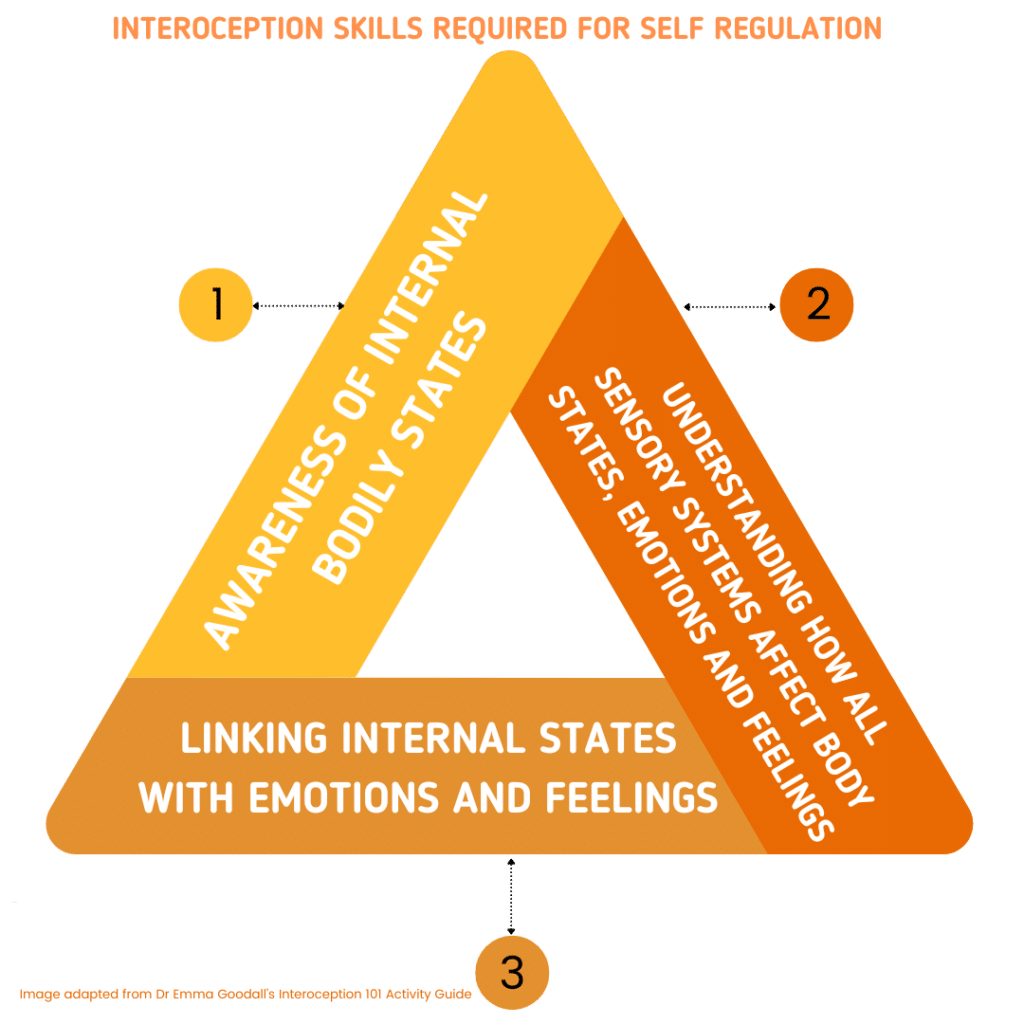
Effective self-regulation involves three steps:
- Awareness of internal bodily states, such as being hungry, cold, or sore.
- Understanding how your sensory systems affect your body, emotions, and feelings by constantly interpreting signals from different sensory inputs such as light, seating position, clothing, and sound.
- And finally, linking internal body states with emotions and feelings, such as recognising that hunger can make you irritable, or prone to lashing out.
These three skills develop from infancy and are linked to parts of the brain which have longer windows of development, through childhood and adolescence. This makes development of interoception particularly susceptible to environmental and relational influences.
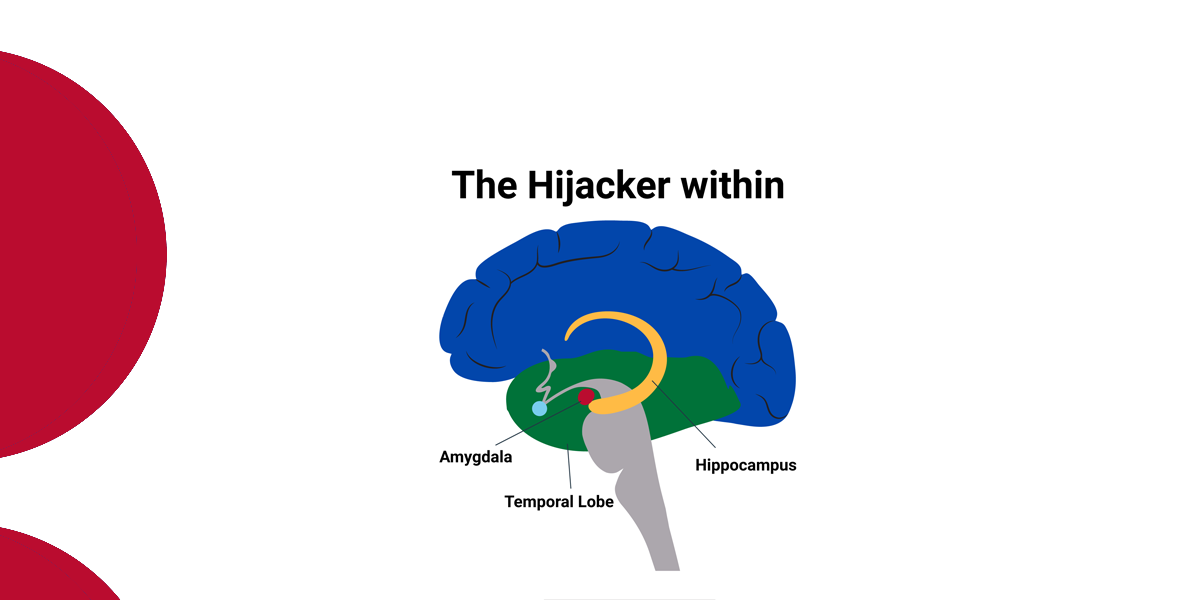
Interoception and relational trauma
There is growing interest in exploring attachment styles, interoception, and related concepts such as alexithymia (also called “emotional blindness”), where someone has difficulty experiencing, identifying, and expressing emotions. The brain regions involved in interoceptive development are also associated with those influenced by attachment processes (Kühn & Gallinat, 2013; Sheffield et al., 2013; Lim et al., 2014).
One recent study found strong correlations between attachment styles and interoceptive awareness (Oldroyd, Pasupathi, & Wainryb, 2019). In this study, anxious attachment was associated with a heightened awareness and worry about internal bodily cues, while avoidant attachment was associated with lower awareness and trust in those cues.
Further unpacking the development of co-regulation and self-regulation, Fonagy (2001) and Stern (1985) theorised that to understand their own mind, children require a sensitive caregiver to reflect it back to them. Oldroyd, Pasupathi, and Wainryb (2019) suggest this is the same for children developing understanding of their own body. For instance, if a child who falls over and feels pain is met by a parent who immediately dismisses it rather than acknowledging the pain and its intensity, the child may learn to dismiss those painful feelings.
This theory was supported in a second study by Oldroyd, Pasupathi, and Wainryb (2019), which measured young people’s physiological responses and self-reported emotions when discussing past life events, alongside their caregivers’ emotional responsivity, across several scales. The study found that caregivers who were less accepting of negative emotions were associated with their young people with less congruent emotional and physiological responses. These young people demonstrated physiological stress responses, but had mismatched emotional states that lacked distress.
Current research suggests that children and young people with relational trauma are more likely to have interoceptive differences, affecting their capacity to notice and respond to internal body cues. Some children may avoid or dismiss cues, while others may be hypervigilant and over-respond to them.
Both groups of children with lower or higher interoceptive awareness may demonstrate their overwhelm and distress in behaviours that their caregivers can find challenging, in either externalising or internalising behaviours can that become significantly more intense during adolescence. Through intentionally noticing a child’s internal bodily experiences and reflecting them back with curiosity, we can help build their capacity to self-regulate.
How do we use this knowledge to help children self-regulate?
The current research underscores what we already know: children and young people with developmental trauma need co-regulation to develop their brain in a “bottom-up” manner – starting with using and regulating their body, before advancing to cognitive processes.
Although research is still evolving, we can already apply these insights in our everyday practice.
")
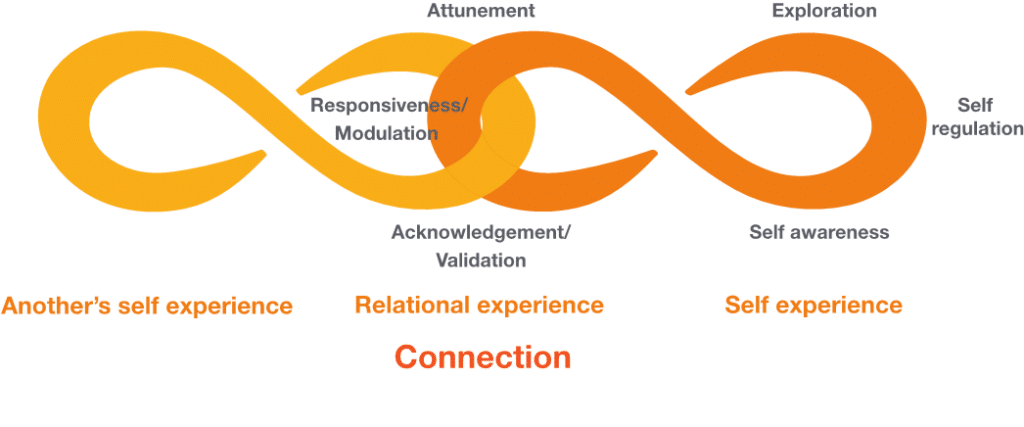
The pathway for self-regulation and co-regulation involves:
- Noticing the internal and external body cues
- Identifying the underlying body state and emotion
- Mobilising to act
- Taking an appropriate action to reduce anxiety.
It is important to remember that before a child, young person, or adult can engage in self-regulation, they first need to understand the internal body cues they are responding to. Many children and young people with interoceptive challenges may be experiencing an overwhelming number of cues by the time they become dysregulated and may be unable to discriminate between them.
Role-modelling your own awareness of internal body cues and feelings and narrating your responses can help guide your child or young person towards finding their own ‘just right’ responses that achieve balance and homeostasis.
Start by becoming aware of your own interoceptive awareness and tuning into your body. Then, develop your own interoceptive language, describing what your body cues feel like and how they relate to your emotions.
If someone is unable to perceive the cue or is overwhelmed by multiple cues occurring at once, it is unlikely that they that will be in a window of tolerance where they can identify the underlying reason and be mobilised to act. For children, the presence of a co-regulator who remains regulated and works through the underlying body state or emotion is crucial. This co-regulator needs to then identify the appropriate action and tolerate the difficult emotion alongside their young person.
This process is the key for the child or young person to learn the process of regulating difficult feelings and developing strategies that support them when those difficult feelings and body states arise.

To find out more about children’s sensory systems and how to tailor co-regulation strategies to children’s individual needs, don’t miss Jessica’s upcoming virtual workshop on attuning to the sensory needs of children and young people in care, for all adults who live with or work with children and young people in care.
Resources
Dr Emma Goodall’s Interoception 101 Activity Guide
https://sies.sa.edu.au/wp-content/uploads/2019/04/Interoception-101_March-2019.pdf
References
Garfinkel, S. N., Tiley, C., O’Keeffe, S., Harrison, N. A., Seth, A. K., & Critchley, H. D. (2016). Discrepancies between dimensions of interoception in autism: Implications for emotion and anxiety. Biological psychology, 114, 117-126.
Kühn, S., and Gallinat, J. (2013). Gray matter correlates of posttraumatic stress disorder: a quantitative meta-analysis. Biol. Psychiatry 73, 70–74. doi: 10.1016/j.biopsych.2012.06.029
Lim, L., Radua, J., and Rubia, K. (2014). Gray matter abnormalities in childhood maltreatment: a voxel-wise meta-analysis. Am. J. Psychiatry 171, 854–863. doi: 10.1176/appi.ajp.2014.13101427
Oldroyd, K., Pasupathi, M., & Wainryb, C. (2019). Social antecedents to the development of interoception: Attachment related processes are associated with interoception. Frontiers in Psychology, 10, 712.
Sheffield, J. M., Williams, L. E., Woodward, N. D., and Heckers, S. (2013). Reduced gray matter volume in psychotic disorder patients with a history of childhood sexual abuse. Schizophr. Res. 143, 185–191. doi: 10.1016/j.schres.2012.10.032