A story you may recognise
Mar 2021
Written by Noel Macnamara
Peta had worked in residential care for 18 months. She took the position because she had had a difficult childhood and she felt that she had a lot to offer the young people in care. She was currently undertaking Cert IV and she was really enjoying it.
There was a new young woman in the ITC house, and she had been having some trouble settling particularly before bedtime. Peta had read a little about Miley and she knew the young women had been passed from kinship care to foster care and in foster care she had a number of different placements. The referral said these moves were due to her behaviours that challenged those who cared for her. At seven years old, she had been removed from her mother and stepfather due to sexual abuse, violence, neglect, and criminal activity in the home. It was suspected that Miley had been made to have sex with the friends of her stepfather for money. Peta almost cried when she first read about Miley, and she had tried every night to spend some time talking to her about her day.
Every night before bed since she arrived, however, Miley would go into a meltdown: throwing things around her room, swearing at staff, and other young people. A week ago, Miley became particularly dysregulated and violent toward another young person, and staff, including Peta, had to intervene to separate the two and keep the other young person safe. As Peta was blocking Miley from getting to the other young person, she started to scream at Peta, “Yeah! that’s right! you just want to touch me up!” while she pulled her top up over her bra, Miley went on to say “you like that don’t you”.
Peta went home shaken and feeling dirty all over. She showered for a long time but when she tried to sleep, she found it very difficult. She kept seeing Miley’s face and hearing her words. Petra was also experiencing frequent headaches. She found herself afraid to talk with Miley and instead stayed distant, simply giving directions. Peta began to wonder if she was as bad as all the adults who had abused or given up on Miley in the past were. She had started to see her fellow staff members as callous and uncaring and had not spoken much to them during the next weeks. over the past week. Peta was tired and frightened to do the work she had felt capable and confident about just a few weeks before.
On a Friday night shift, as the noise in the Miley’s room escalated, Peta froze, just staring at Miley screaming and grabbing and throwing things around her room. Her coworker mumbled as he walked by her into the room, “Here we go again” Peta’s stomach was filled with butterflies as she followed him in to try to calm Miley down and get her settled for the night.
In a team meeting the following week Peta found herself putting forward an argument that this might not be the right place for Miley.
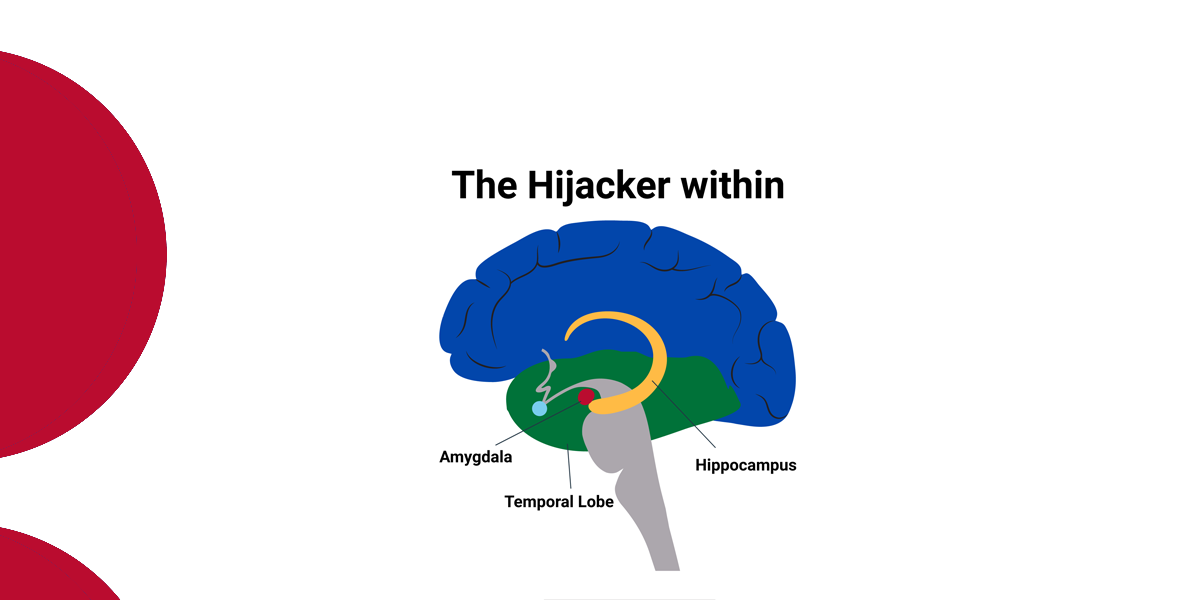
This story describes a youth worker’s reaction to a common scenario in residential services all across Australia. Peta’s reaction to the experience she had with Miley, including intrusive recollections, disturbed sleep, fear and reluctance to engage with Peta after the incident, withdrawal and negative perceptions of her team members and a punitive response to Miley can be characterised as secondary stress or compassion fatigue.
Figley (2002) defines compassion fatigue as “a state of tension and preoccupation with the traumatised client by re-experiencing the traumatic events, avoidance/numbing of reminders, [and] persistent arousal (e.g., anxiety) associated with the client. It is a function of bearing witness to the suffering of others” (Figley, 2002, p. 1435). Unlike burnout, which emerges gradually because of emotional exhaustion, compassion fatigue can emerge suddenly as in the case of Peta.
Compassion fatigue includes a sense of helplessness, isolation, and confusion, which may be disconnected from specific triggers. Pearlman and Saakvitne (1995) emphasise that compassion fatigue involves the symptomatic presentation of the caregiver of traumatised/distressed clients as a result of exposure to the clients’ trauma. Compassion fatigue as a phenomenon very much resembles the symptomatic presentation of posttraumatic stress disorder (PTSD; American Psychiatric Association, 2000).
There is hope
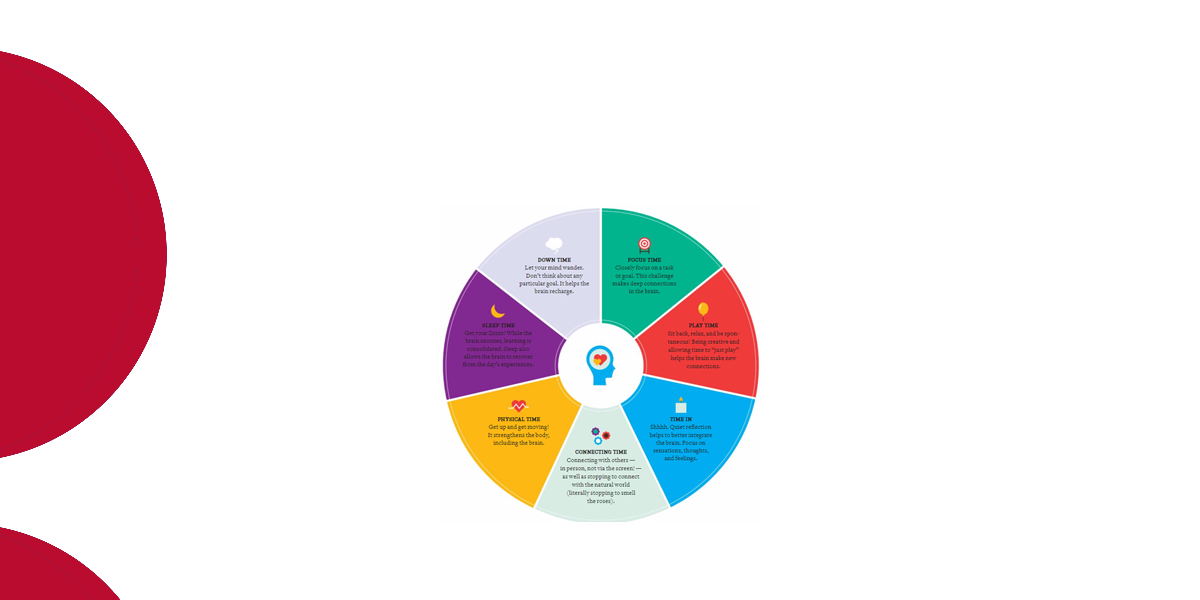
If you see shades of yourself in Peta, don’t worry. Relief is actually nearby. To recharge your batteries, you must first learn to recognise when you are being impacted and then get into the habit of doing something every day that will replenish you. That’s not as easy as it sounds. Old habits are oddly comfortable even when they’re bad for us, and real lifestyle changes take time (some experts say six months).
|
DO |
DON’T |
| Talk with your supervisor | Blame others/young people |
| Engage in reflective practice | Look for a new job |
| Understand that the pain you feel is normal. | Fall into the habit of whinging with teammates |
| Start exercising and eating properly. | Work harder and longer |
| Get enough sleep. | Self-medicate |
| Take some time off | Neglect your own needs and interests |
| Develop interests outside of work. | |
| Identify what’s important to you |
Most staff come into residential work wanting to help young people and they have an idea of how it’s going to look when they help someone, but sometimes it doesn’t go according to how they think it should go. This dissonance can contribute to compassion fatigue.
An organisational culture that gives permission and provides a safe space for staff to talk openly about the work and the impact of the work is an antidote for emerging compassion fatigue. Along with good recruitment and on-boarding practices, regular reflective practice sessions and trauma informed supervision are essential for all of us engaged in trauma work.