How do you support staff feeling defeated and powerless? A Case Study
Nov 2020
Written by Tram Nguyen
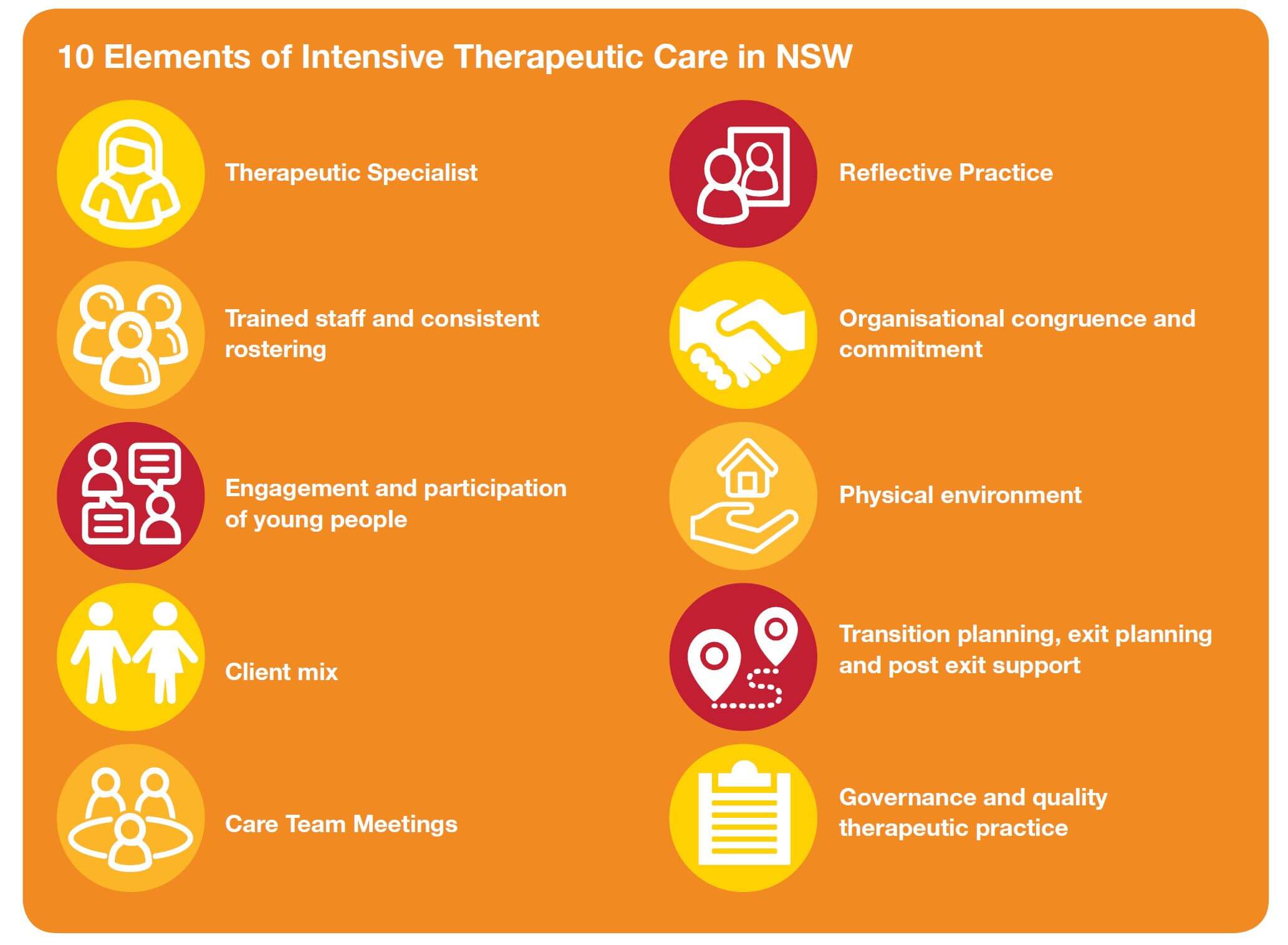
My work as a Therapeutic Specialist is about finding ways to equip and support staff to provide high-quality therapeutic care for young people living in Intensive Therapeutic Care homes.
It is about sharing knowledge, facilitating reflective practice and, perhaps most importantly, holding the hope that positive change is possible.
In this blog, I want to share a story about a young woman – de-identified and anonymised for confidentiality – who’s behaviours challenged our team to stay hopeful in the face of complex trauma and pain.
The Case Study
Katrina grew up in Wagga, where she and her family had significant ties and relationships. When she was 9 years old, Katrina was put into state care by her birth mother. She went on to experience numerous foster placement breakdowns, eventually being placed in an Intensive Therapeutic Care Home (ITCH) in the Sydney area at 12 years of age.
Katrina was moved out of a 4-bedroom ITCH house after a couple of years and into a 1:1 placement due to increased violence and risk of harm to other young people. Katrina did not respond well to this transition and expressed to her care team that her sense of abandonment and reaction was more painful than when she was placed in state care by her mother.
Katrina was diagnosed with ADHD and RAD diagnoses and was often not compliant with her medication and resistant to psychological supports. Katrina presented with sexualized behaviours and was at risk of sexual exploitation. Her care team were aware that Katrina was meeting older men in the community who were providing her with alcohol and other drugs.
Katrina’s care team were finding it difficult to connect with Katrina due to her extreme intimidating and at times, frightening behaviours. This included: verbal and physical abuse directed at staff. At one moment, Katrina went through cycles of seeking closeness and relationship with staff, and then pushing the staff away and attempting to destroy the relationship through verbal and physical aggression.
Katrina’s care team would often raise these issues in reflective practice sessions. They said they felt powerless and hopeless about what could help her. They felt as if they were failing Katrina and were unable to create any positive change, as the behaviours of concern and risk continued to increase despite being in a 1:1 on placement.
As the Therapeutic Specialist tasked with providing advice and support around the best therapeutic care approach, I also found myself feeling defeated. I felt backed into a corner at times when the care team and other professionals, such as DCJ, school and management, were seeking answers. I did not have ‘magic wand’ and was struggling to navigate a path forward that would resource Katrina and her staff team best.
How did I respond?
Reflective Practice: Our fortnightly reflective practice session provided a critical space for us to discuss, analyse and review feelings, approaches, strengths and worries.
Care Team Meetings: The care team meetings allowed us to think and plan collaboratively with other professionals and services that wrapped around Katrina and her experience in care. There were multiple services involved with Katrina and it was essential that we collaborated and remained focused on what Katrina needs were.
Regular communication with the house manager and case manager: Being in regular communication with Katrina’s house manager and case manager was critical to continue thinking, planning and reviewing together, while also building their collective resilience to working with Katrina.
Offering psychological first aid: It was important to offer psychological first aid and debriefing with individual staff and the broader team after a crises situation. This helped ground the staff members and allowed them to continue to offer trauma-informed care for Katrina.
What grounded me?
Monthly Community of Practice: Being able to participate and gain professional guidance and support from the CETCs monthly Therapeutic Specialist Community of Practice was really helpful. I found the process of sharing Katrina’s story helped to ground me and feel connected to my other Therapeutic Specialist colleagues beyond my immediate agency. The CoPs are a shared community of learning and growing together. Sharing with my colleagues it was helpful to recognise that the challenges we face are highly complex and do have ‘quick-fix’ answers.
Being open and accepting my gaps and vulnerability: I’m not the ‘expert’ with all the answers, and I am OK with that. I also recognized that I cannot and should not be expected to ‘hold’ the emotional and psychological needs of staff in the context of working with complex trauma, but I can and do create spaces for reflection, capacity building and ongoing support.
Supervision (formal and informal): Supervision was a place to go and not have to know the answers, A place to work things out. It’s also a place to be reassured, supported, and somewhere to take the emotional disturbance of the work. A place where I could share and be understood and reflect and to receive helpful and constructive feedback.