Frequently asked questions by foster carers: Behaviours that challenge
Jun 2022
Written by Noel Macnamara
In Australia, there are about 18 thousand children and young people in foster care. Most foster carers will be the first to tell you how rewarding it is – but it is also challenging, tiring, and sometimes distressing.
Children and young people in out-of-home care often have early adverse life experiences resulting in trauma-based behaviours. Foster carers can find these behaviours alarming, uncontrollable, unpredictable, and even inexplicable.
How trauma can affect children |
|
| Bodily | • Uncontrollable physical responses to stress
• Chronic illnesses (e.g. heart disease, obesity), even into adulthood |
| Cognitively | • Difficulty thinking, learning, and concentrating
• Impaired memory • Difficulty switching from one thought or activity to another |
| Emotionally | • Low self-esteem
• Feeling unsafe • Inability to regulate emotions • Difficulty forming attachments to caregivers • Trouble with friendships • Trust issues • Depression, anxiety |
| Behaviourally | • Lack of impulse control
• Fighting, aggression, running away • Substance abuse • Suicide, self-harm |
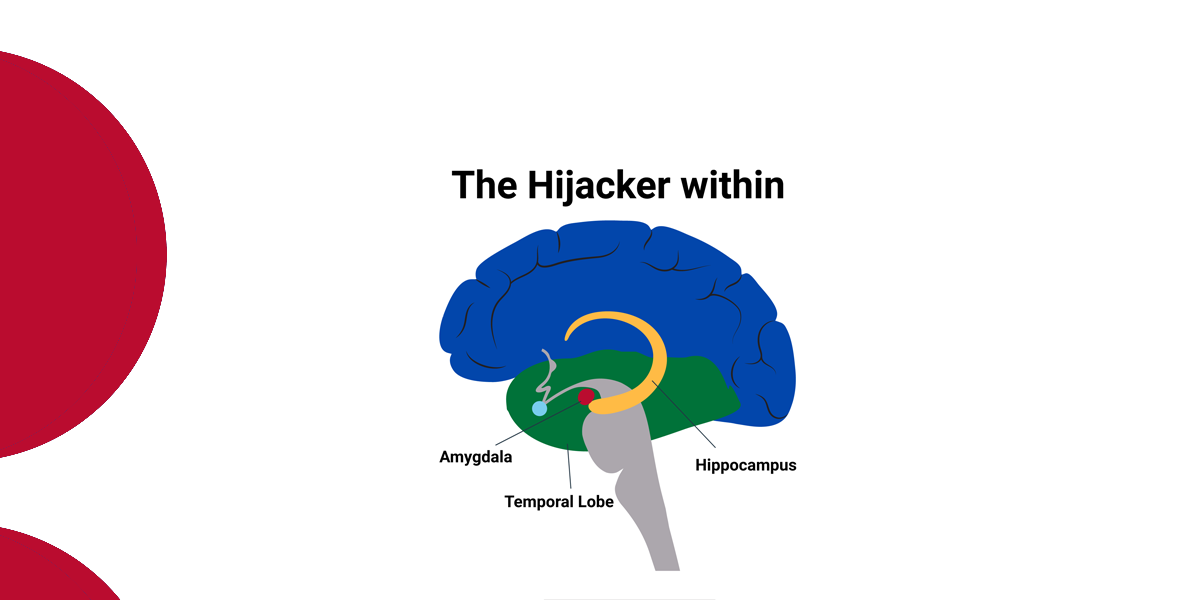
Some of my colleagues use the metaphor of falling into a ‘time hole’ to illustrate children’s sudden mood changes accompanied by extreme behavioural difficulties. These behaviours may be externalised (aggressive/controlling) and/or internalised (dissociative/rejecting).
Some stories of confusion that carers have shared with me:
“I bought both children a toy. The next day I found both toys shoved under one boy’s bed. When I asked him about it, he said he wanted to leave and told me to call his worker.”
“He stole the jewellery that my mother left me when she died. When I asked him why, he swore at me and said I deserved it.”
“She went into my bedroom and cut up my wedding dress and then denied it.”
“When I was unwell, she became so demanding. Telling me to get up. Asking for special foods to be made. Getting angry.”
“There had been no problems, we were getting along really well. Then one night, she sneaked out and was missing for three days.”
In the table below, I have included some common signs of trauma in children of different age groups.
Common Signs of Trauma in Children of Different Age Groups |
||
| Young Children
(Ages 0–5) |
School-Age Children
(Ages 6–12) |
Teens
(Ages 13–18) |
| •Irritability, “fussiness”
•Startling easily or being difficult to calm •Frequent tantrums •Clinginess, reluctance to explore the world •Activity levels that are much higher or lower than peers •Repeating traumatic events over and over in dramatic play or conversation •Delays in reaching physical, language, or other milestones |
•Difficulty paying attention
•Being quiet or withdrawn •Frequent tears or sadness •Talking often about scary feelings and ideas •Difficulty transitioning from one activity to the next •Fighting with peers or adults •Changes in school performance •Wanting to be left alone •Eating much more or less than peers •Getting into trouble at home or school •Frequent headaches or stomach-aches with no apparent cause •Behaviours common to younger children (thumb sucking, bed wetting, fear of the dark) |
•Talking about the trauma constantly, or denying that it happened
•Refusal to follow rules, or talking back frequently •Being tired all the time, sleeping much more (or less) than peers, nightmares •Risky behaviours •Fighting •Not wanting to spend time with friends •Using drugs or alcohol, running away from home, or getting into trouble with the law |
The foster carers I know and have worked with recognise these needs. However, given the complexity of many children’s behaviour, they can feel overwhelmed, unprepared. This is understandable given this is outside the realm of ‘ordinary’ parenting. Thus, fostering can involve high levels of stress, compassion fatigue, secondary traumatic stress, and personal sacrifice.
In my opinion not enough attention has been given to understanding the impact on foster carers of caring for abused and traumatised children. In this series of blogs, I will unpack some key issues that, in my experience, have a very significant impact on foster carers.
How do I manage behaviours that challenge?
Our first and most frequently asked question: how do I manage behaviours that challenge? The children in foster care are complex individuals with complex needs and backgrounds. Sometimes, to come to terms with what they’ve been through, children manifest these needs in the form of seemingly antisocial or self-destructive behaviours. Such as violence and tantrums, self-harm and running away from home and getting into trouble with police.
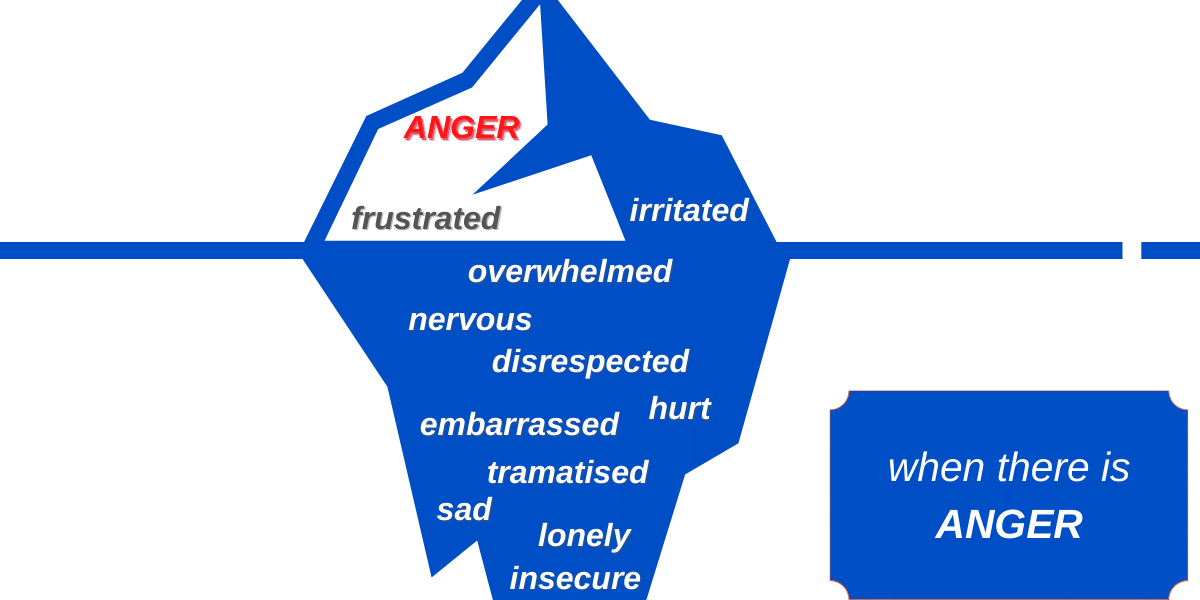
As a child or young person who has experienced trauma attempts to avoid feeling unsafe, a lack of trust or the pain of rejection, the way they communicate is often the opposite of what they really need. For example:
| When a child or young person appears to communicate… | Consider what else this might communicate… |
| I DON’T NEED COMFORT | I can’t let myself be vulnerable |
| I DON’T NEED SUPPORT FROM YOU | I can only rely on myself |
| I DON’T TRUST YOU | I have learnt that adults aren’t trustworthy |
| I AM NOT SAD | I don’t know what I feel |
| I AM FINE | If you know how I feel, you could use it to hurt me |
| I DON’T TURN TO YOU FOR HAPPINESS OR COMFORT | Feeling happy makes me aware of what I have missed |
| I DON’T WANT TO SPEND TIME WITH YOU | If I let our bond strengthen, it will hurt more when you finally reject me |
Questions to ask of behaviours that challenge
Consider the following story:
Graham was 10 years old when he was placed with Mrs Brown. When Graham first arrived, everything seemed to go pretty well, except for sleeping. Graham would get under his bed and hardly slept at all. Mrs Brown was perpetually exhausted from repeatedly putting Graham back in bed, quietening him down, and telling him he was safe.
As the weeks went on things began to get worse. Graham was verbally abusive to the other children and tried to hurt them. He was very frightened. He soiled himself and smeared his faeces. He urinated everywhere. He ripped furniture and bedding. When the Browns took Graham away to their holiday home, he tried to set it on fire. He threw food and would not eat. One time, he pointed a large knife at Mrs Brown.
To help children like Graham deal with what he is going through, it’s important to consider the potential reasons behind these behaviours.
Try these questions:
-
1. What happened to Graham?
If you find yourself asking “what’s wrong with Graham?”, try correcting yourself to “what happened to Graham?” Graham’s child protection worker and your foster care worker should provide you with as much information as they can to be able to care for Graham appropriately. Knowing all you can about his history will assist you to anticipate and meet his safety needs. We have historically thought of “safety” as simply the absence of abuse and neglect, and that type of safety is a critical first step on the road to well-being. However, safety also includes the concept of feeling safe; a concept called “psychological safety”. We cannot feel a sense of well-being without feeling safe first. Caring for a traumatised child or young person may require a shift from seeing a “bad kid” to seeing a kid who has had bad things happen.Graham’s History
Graham’s father was very violent, particularly at night when he returned from the pub. Graham’s mother would wrap him up in a doona and put him under the bed to protect him. Graham would put his fingers in his ears and sing. Graham survived.
Mrs Brown, through her desire to care for Graham, had unknowingly increased his anxiety, fear, and lack of psychological safety by removing him from under the bed where Graham believed was safe.
-
2. What does Graham’s behaviour mean?
For Graham, “safety” was being wrapped-up under his bed, blocking out the noise of his father’s violence. Although Graham had left his family home, his safety system remained.
-
3. What is Graham trying to communicate?
Perhaps, “I am unsafe, so I need to do the things I do to feel safer, until I do feel safe, if I ever do. I do not know how to trust or who to trust.”
-
4. What does the behaviour feel like on the inside for Graham?
Perhaps, “I might die. I might hear someone else die.”
-
5. How should you react to Graham’s behaviours?
Graham has behaviours that he feels keep him alive. We must respect these and allow him to make use of them until his brain tells him that he does not need them any longer. We can only reassure Graham that sleeping in his doona is safe, until he learns to trust his carers and his environment are safe. Safety always comes before trust.
As caring adults, we must stay curious and help children identify things that instil the feeling of safety, and eliminate or minimise things that can cause feeling unsafe. Help the child to make sense of his/her behaviour by naming hidden feelings causing the behaviour, and responding to them in a calming and safe way. Over time, this help children repair from trauma.
Are you getting the support you need?
As a foster carer who is caring for a child or young person it is so important to take care of yourself and recognise the risks of compassion fatigue (Blocked Care) and vicarious trauma. In a later blog in this series, we will look at this issue.
As a foster carer, you also require emotional and educational support from your agency/government department. Those supports must specifically relate to understanding and managing the issues experienced by the child(ren) in your care. In the next part of this blog series we will explore the issue of support.
References
- Baylin, J., & Hughes, D. (2016). The neurobiology of attachment-focused therapy (pp. 1 to 16). New York: W.W. Norton & Company.
- Sinclair, I. (2005). Foster Children: Where They Go and How They Get on. United Kingdom: Jessica Kingsley Publishers.